
Induced After‑Death Communication (IADC) has quietly moved from the fringes toward the clinical mainstream. It began as a modification of EMDR, but the more recent work treats it as its own experiential grief therapy, focused less on trauma replay and more on opening a very particular state of consciousness where contact with the deceased may arise. In current clinical studies, IADC is now framed as a brief, brain‑based approach that helps people enter a receptive, grief‑specific state in which vivid, often life‑changing “visits” from loved ones occur—and those visits are strongly linked with reduced grief, more peace, and an ongoing, healthy sense of connection.
A recent observational study comparing IADC to standard grief work (talk therapy plus EMDR) found that IADC clients not only improved faster, but also felt a stronger, more adaptive continuing bond with the person who died, along with higher satisfaction with therapy. Another study looked at what actually happens in IADC sessions and found that the great majority of experiences meet criteria for near‑death experience–like states: profound peace, encounters with deceased loved ones, and a sense of otherworldly environments. In other words, IADC seems to reliably invite people into a non‑ordinary state of consciousness that looks a lot like what is reported in classic NDEs.
At the same time, research on spontaneous after‑death communication (ADC) keeps saying the same thing: these experiences are common, often cherished, and usually healing. Large international surveys show that ADCs tend to reduce fear of death, increase spirituality, and become a turning point in someone’s grief story. Another mixed‑methods study found that those who report ADCs tend to show higher gratitude and compassion, and describe the experience as a catalyst for “good grief”—a grief that transforms rather than just wounds.
Havening, Soothing Touch, and “Brains that Listen”
Havening Techniques® use gentle, rhythmic touch combined with specific mental focus. The touch is designed to stimulate the skin’s affective touch system—special nerve fibers that respond to slow, caring contact. A recent review of touch‑based therapies suggests that this type of touch can calm stress systems, change how the brain processes threat, and improve interoception (our felt sense of the body). Havening theory goes further and proposes that this soothing input, when paired with emotional material, can help “depotentiate” the neural circuits that keep traumatic feelings stuck.
While the science on Havening is still early, case reports and theoretical work point in the same direction: rhythmic, pleasant touch plus focused attention can shift the brain into a calmer, more integrated mode. Many practitioners (myself included) notice that in this softened state, clients sometimes “slip” into experiences of deep connection—memories, meaningful imagery, and at times unexpected encounters with those who have died. That was exactly what I witnessed: while using Havening for things like eating patterns or chronic pain (not explicitly grief work), clients spontaneously reported clear, emotionally rich visits from a deceased mother or friend.
From a research perspective, this is very much in line with what we see in IADC and other ADC‑oriented modalities:
- A safe, guided container
- A deeply relaxed yet focused state
- A willingness to be emotionally open
- Some form of rhythmic sensory input (eye movements, touch, visual focus, etc.)
Put together, these elements seem to invite the mind into a threshold state where connection feels not only possible but natural. Whether one frames this as brain‑based imagery, genuine communication, or both, the emotional impact is real: relief, peace, love, and a softer relationship with grief.
Chanting, Rhythm, and Mystical Brain States
Now let’s bring in chanting, because this is where the “brainwave” and “beyond‑the‑veil” themes really start to weave together.
Gemma Perry and colleagues have been doing some of the most interesting work here. In a large global survey of people who regularly chant across 33 countries and many traditions, about 60% reported full‑blown mystical states: deep peace, unity, and experiences that felt impossible to put into words. It didn’t matter whether the chanting was vocal or silent, solo or in a group, or which tradition it came from—mystical experiences showed up across the board. What did matter was absorption (the ability to become fully immersed), altruism, and religiosity: people who tend to “lose themselves” in an activity and who approach chanting with devotion and intention were more likely to have mystical states.
Another study by the same group went deeper into what chanting actually does psychologically. Stronger intention (devotion, meaning, focus on sound) and greater engagement (experience, regularity, length of practice) were associated with:
- More flow (that timeless, effortless absorption)
- More mystical experiences
- Better mindfulness and less mind‑wandering
- Better quality of life, indirectly, through these altered states
And in an experimental study on online chanting, experienced chanters who did just 10 minutes of chanting showed more ego‑dissolution (the sense that the small “me” has loosened) and more mystical experience than those who simply listened to a narrative; spirituality also shaped how powerful these states felt.
From the acoustic side, another team analyzed chants from seven global traditions and found they share surprisingly similar sound features: relatively flat, slow‑changing pitch, smooth and continuous voicing, and a comfortable, low pitch range. When people listened to recordings engineered to include these exact acoustic features, they consistently reported more relaxation. The body likes this kind of sound—vocal tracts relax, and listeners feel soothed.
A broader neurobiological review of rhythmic sound practices—shamanic drumming, chanting, rhythmic sonic patterns—pulls this together:
- Rhythmic repetition tends to induce absorption and relaxation.
- The brain appears to entrain to low‑frequency patterns, shifting large networks into slower, more synchronized modes that resemble other altered states (including psychedelic and psychotic states, but also deep meditative and mystical states).
In plain language: rhythm pulls the brain into a different gear.
Threshold States: IADC, NDEs, Chanting, and Mystical Contact
When we zoom out, a pattern emerges across very different contexts:
- IADC therapy: Carefully guided, emotionally focused, with bilateral stimulation; many clients report encounters with deceased loved ones that score high on near‑death experience–like scales.
- Spontaneous ADCs: Often emerge in dreams, quiet moments, or times of inner stillness and longing, and are usually comforting, strengthening, and spiritually meaningful.
- Meditation‑induced ADC (MI‑ADC): Conceptual work suggests meditation is well‑suited to evoking after‑death contact, especially when it emphasizes relaxation, receptivity, visual imagery, and gentle guidance.
- Chanting and rhythmic sound: Across cultures, rhythm and repetition draw people into mystical states, ego‑dissolution, and profound peace.
- Near‑death experiences: Modern neuroscience finds bursts of highly integrated brain activity and complex oscillations around the time of clinical death, correlated with classical reports of light, beings, and other realms.
None of these studies can “prove” what is happening ontologically—whether consciousness is leaving the body, whether the deceased are truly present, or whether the brain is generating a healing inner drama. Researchers are increasingly careful to separate the experience (which they can measure) from the ultimate explanation (which remains open).
But they consistently find three important things:
- These experiences are normal, not rare. ADCs, NDE‑like events, and chanting‑induced mystical states show up all over the world, in ordinary people.
- They are usually helpful. Less fear of death, more spirituality, more meaning, more gratitude and compassion, and often a more peaceful relationship to loss.
- They arise in specific mind‑body conditions. Safety, emotional openness, rhythmic and/or soothing sensory input (touch, sound, visual focus), and a willingness to enter a relaxed yet attentive, imaginative state.
This is exactly the territory where my accidental “Beyond the Veil” work lives:
- Havening Touch® to calm the nervous system and gently unwind traumatic charge.
- Imagination and intention to lean into love, grief, and the felt presence of the person who died.
- A facilitator who trusts the process and honors whatever arises without forcing a particular belief.
From the vantage point of current research, this is not “out there.” It is a creative, heart‑forward application of what is increasingly recognized: when the body is soothed, the brain shifts into slower, more integrative rhythms, and the heart is open, humans naturally enter states where connection beyond the veil feels close, real, and deeply healing.
The science cannot yet tell us what you are touching beyond that veil. But it can absolutely support the idea that building safe, structured ways to explore these states—with touch, rhythm, imagery, and love—may be one of the most powerful gifts we can offer the grieving.
My Research
With a small group of volunteers, I developed a method that demonstrated an 87.5% success rate in facilitating beyond-the-veil communication. The approach integrates Havening Techniques® (known for creating healing delta brain waves) for initial emotional depotentiation and imaginative practices (correlated with theta brain wave generation).
At the heart of BTV communication is a tender acknowledgment that grief, as I like to say, is “love turned inside out.” I’ve come to view this also like peeling back an onion (EXAMPLE BELOW):
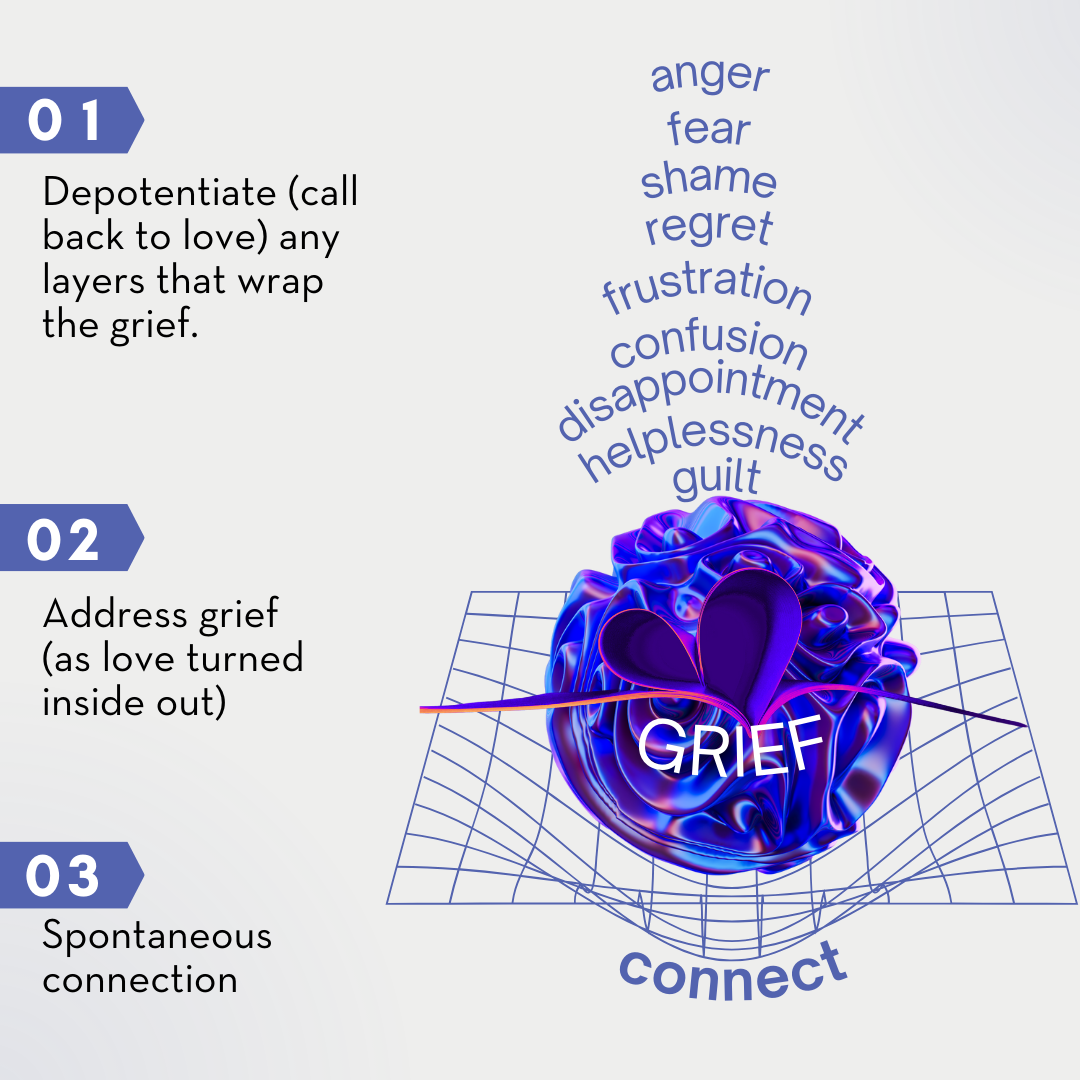
Once we depotentiate the outer layers of the onion with Havening Techniques®, we get to grief as love, turned inside out. The client explores this beautiful love with a process involving imagination.
This is not a specific order to follow — I help the client go in the order they wish. I am merely a facilitator. Grief is typically “wrapped” in a mixed bag of emotions. The emotional mix confuses and troubles us. The loss of a loved one can surface deep feelings of shame and guilt. Shame often stems from regrets over unresolved issues (including the resurfacing of past issues long “forgotten”), perceived failings in the relationship, feelings of responsibility for the death, anger, relief, or benefiting from the loss (inheritance). Again, the above onion is an illustrative example to show this metaphor of peeling back the grief onion. THIS IS NOT A PRESCRIPTIVE, SEQUENTIAL LIST.
UPDATE:
With the help of a MUSE device and some volunteers, I found that touching my head elicited the most delta waves. I have heard this is common. For another volunteer, touching her face elicited the most delta waves. This means that you can try to connect without using Havening Techniques®. My recommendation* would be to make sure your body is in the physiology of safety and connection. Then try touching your face and head (gently) and then use your imagination to picture a pleasant meeting area that is welcoming.
This recommendation is for entertainment and wellness purposes only. I work with wellness, betterment, and “derailers,” NOT disorders. If you might have or have a disorder, connect with your medical professional.
Sources
- D’Antoni, F. et al. (2025). Induced After-Death Communication (IADC) Therapy: An Effective and Quick Intervention to Cope with Grief. Psychology International.
- Lalla, C., & D’Antoni, F. (2025). Induced After-Death Communication (IADC) Experience and Near-Death Experience (NDE): Two Variations of a Single Phenomenon. Psychology International.
- Elfers, J. et al. (2025). Good Grief! After-Death Communication, Grief, and Gratitude. Religions.
- Wassie, N. (2022). Meditation-Induced After Death Communication: A Contemporary Modality for Grief Therapy. International Journal of Transpersonal Studies.
- Penberthy, J. K. et al. (2021). Factors Moderating the Impact of After Death Communications on Beliefs and Spirituality. OMEGA.
- Pait, K. C. et al. (2023). After-Death Communication: Issues of Nondisclosure and Implications for Treatment. Religions.
- Valdez, C., Jordan, J. R., & Botkin, A. (2021). Induced After-Death Communication. In New Techniques of Grief Therapy.
- Costa, M. A., & Moreira-Almeida, A. (2025). Life after death and mind beyond the brain: Reflections and implications for aging. International Psychogeriatrics.
- Barney, K. A., & Yoshimura, S. M. (2020). Death-Related Grief and Disenfranchised Identity: A Communication Approach. Review of Communication Research.
- Crowther, S. et al. (2025). Havening: a psycho-sensory therapy for enhancing emotional resilience and psycho-emotional wellbeing across the perinatal period. Frontiers in Global Women’s Health.
- Papi, M. et al. (2025). The role of affective touch in mental illness: a systematic review of CT fiber dysregulation and therapeutic potential. Frontiers in Psychiatry.
- Perry, G., Polito, V., & Thompson, W. F. (2021). Rhythmic Chanting and Mystical States across Traditions. Brain Sciences.
- Perry, G. et al. (2022). How Chanting Relates to Cognitive Function, Altered States and Quality of Life. Brain Sciences.
- Perry, G. et al. (2025). Altered states of consciousness induced by online chanting meditation. Current Psychology.
- Canessa-Pollard, V. et al. (2025). Chants across seven traditions share acoustic traits that enhance subjective relaxation. PNAS.
- Aparicio-Terrés, R. et al. (2025). The neurobiology of altered states of consciousness induced by drumming and other rhythmic sound patterns. Annals of the New York Academy of Sciences.
- Mashour, G. et al. (2024). Consciousness and the Dying Brain. Anesthesiology.
- Simamora, S. L. et al. (2024). Transcendental Communication with Near Death Experience. COMMICAST.